Why There’s A Bright Future for PET/CT
Physicians have realized the value of PET/CT for cancer patients and want to use this imaging modality for all solid tumors. Medicare proposed a Coverage with Evidence Development (CED) trial program that began in 2006 and went until 2009. The results were more then what the PET community anticipated, with an average of 36 percent of change in management. With such great results, coverage was expanded in 2009, but it was not until 2013 that the Centers for Medicare and Medicaid Services ruled that all solid tumors except for prostate cancer will be covered for staging, and all solid tumors including prostate cancer for restaging. The caveat was the patient could have one PET/CT scan prior to treatment and no more than three post-treatment. This rule has since been updated to include that if a patient has a recurrence and more treatment is needed they may have more than the three post-treatment scans.
When Do I Order a Fluorodeoxyglucose (FDG) PET/CT?
- Staging: PET/CT is more sensitive than CT for most aggressive solid tumor types and lymphoma. Therefore, anytime there is a moderate to high probability for M disease PET/CT is the recommended technology. Additionally, when the N status of a patient is difficult to assess surgically (internal mammary lymph nodes, mediastinal lymph nodes, retroperitoneal nodes) PET/CT will be more sensitive than CT.
- Response to Therapy/Restaging: In respect to PET/CT there are a few considerations. We tend to think of lymphomas differently than solid tumors, and solid tumors can be further broken down into neoadjuvant assessment, and those solid tumors that have metastasized and are undergoing systemic chemotherapy response assessments.
Lymphoma: Earlier assessment is better than delaying the assessment. Therefore, an assessment is recommended after one to two cycles of chemotherapy. After the fourth cycle PET begins to lose sensitivity and therefore the negative predictive value of PET/CT. The one caveat is in lymphomas where the staging study is negative as described above. The response criteria is normal, minimal residual uptake and a positive study. Positive studies portend a poor prognosis, irrespective of the degree of positivity; however, there will be a spectrum of positive studies ranging from progression to dramatic response from baseline but still positive. The National Comprehensive Cancer Network guidelines have complete response criteria that should be adhered to for the interpreting radiologist. Those guidelines can be found at www.nccn.org.22-25.
Solid Tumors, Metastatic Disease: The typical timing sequence here will be after two to three cycles of systemic chemotherapy. The additional cycle timing is due to the fact that most tumors respond to cytotoxic chemotherapy at a slower rate compared to liquid tumors (for example, lymphoma). Degree of response does provide some prognostic value and clear progression of disease will provide data necessary to consider a change in therapy.
- Neoadjuvant Response Assessment: There are two considerations when using FDG PET/CT to assess response in a patient undergoing neoadjuvant therapy. First, in those patients that are clinically responding to systemic chemotherapy/radiation most clinicians will use PET/CT after the completion of therapy to gain prognostic data prior to surgical management. Second, in those patients that have clinical signs or symptoms of early progression PET/CT should be considered earlier, after two to three cycles, as a progressive study will lead to considerations of alternate therapy.
- Bone Dominant or Bone Exclusive Disease Is a Consideration: In patients with bone-exclusive disease the response assessment with PET/CT will need to be performed off bone marrow stimulants (GCSF or other agents), as performance on these medications will preclude an accurate assessment. PET/CT should be ordered at least three weeks after the last dose of these medications.
Recurrence: Consider ordering PET/CT on patients with a suspicion of recurrent disease based on symptoms, tumor markers laboratory evaluation or other imaging procedures, and a history of any FDG-avid tumor (aggressive, solid), or lymphoma.
Solitary Pulmonary Nodule (SPN): Is the most widely used indication for FDG PET/CT. Prior to PET/CT, patients that had an SPN on a CT scan had two options. If it was too small to perform a biopsy then the patient would have interval CT scans until it was large enough to biopsy. If it was large enough to biopsy the patient would go through an invasive procedure that may not have been necessary.
Today, if a patient has an SPN that is large enough to image – 6mm up to 3cm – the patient can have a PET/CT to determine if a biopsy is necessary. The negative predictive value of a PET/CT for a nodule that is 1cm or larger is 99.9 percent. This study has helped prevent unnecessary procedures.
~~~
PET/CT is evolving rapidly and there are new isotopes available now, and many more coming soon. Amyloid imaging is available for Alzheimer’s disease but is currently not paid for. A second CED study beginning this year will make this available, and the outcomes hopefully will be beneficial, making this a new indication. There is a Gallium product commercially available for neuroendocrine tumors (Netspot®). There are also new prostate imaging agents available now, and more imaging agents to come this year which will allow imaging of prostate cancer patients to find recurrence much earlier where the outcomes will improve.
Theranostics (therapy with a diagnostic agent): This is where PET/CT is heading – using an imaging agent followed by targeted therapy. Most of these new agents will also have targeted therapies available, providing better outcomes. Today, for example, patients with certain neuroendocrine tumors have limited treatment options. If these patients are imaged with Gallium Netspot on a PET/CT scanner and they fit certain criteria, they can then be treated with Lutathera®. This is the beginning of theranostics. You will see this method of treatment grow rapidly in the near future, and PET/CT will play a huge part in this.
How to Order an FDG PET/CT
When a patient requires a FDG PET/CT, trust Cooper University Health Care’s radiology experts. At Cooper Radiology we conduct a wide array of screenings and imaging exams for men, women, and children to diagnose any existing conditions.
When your patient’s health requires a closer look, schedule a visit with Cooper Radiology.
Call 888.499.8779, or schedule online.
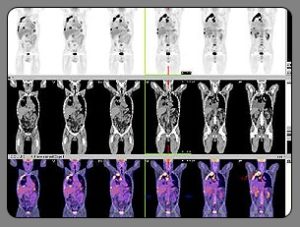
Details of the three types of scans: Top row: PET; middle row: CT; bottom row: PET/CT